Heterotopic pregnancy
Article Published: May 24, 2002
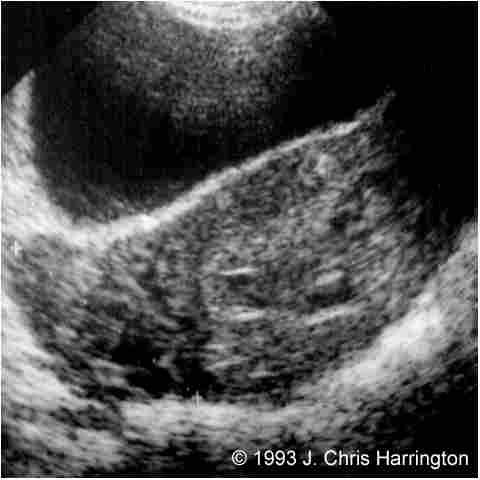
Figure 4: Transverse transabdominal scan showing a right adnexal mass (calipers).
In addition, there was also a moderate amount of free intraperitoneal fluid. Again, the mass was thought to most likely represent a hemorrhagic corpus luteum, and a follow‑up examination was ordered.
Two weeks later the patient returned for the follow‑up examination and related a history of increasing right‑sided pain. She had not had any bleeding. A transabdominal and transvaginal scan revealed a single live normal intrauterine pregnancy, demonstrating appropriate interval growth with a CRL of 32mm, consistent with a menstrual age of 10 weeks (fig. 5).
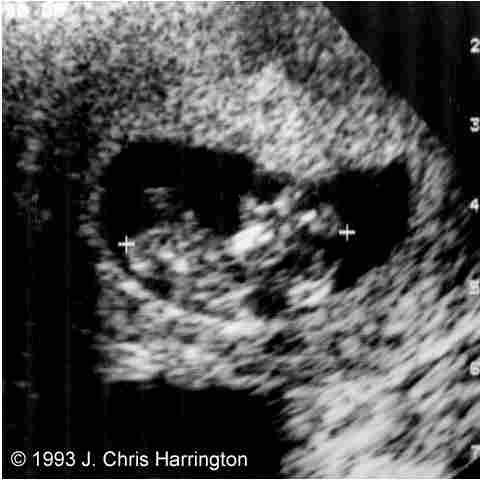
Figure 5: Transverse scan showing a 10 week intrauterine gestation.
Note was made of a small extrachorionic fluid collection. The left adnexa was normal. The right‑ sided mass was again identified and now measured 90 x 50mm (fig. 6). A small amount of free fluid was present.

A differential diagnosis of hematoma, inflammatory reaction or ectopic pregnancy was given.
In light of the patient"s persistent pain, a laparotomy was scheduled and at surgery a ruptured ampullary right ectopic pregnancy was found. A right salpingectomy was performed. There was minimal blood loss during surgery, and the postoperative course was unremarkable. Pathologic examination of the surgical specimen revealed the presence of chorionic villi and confirmed the diagnosis of a ruptured right ectopic pregnancy. The remaining pregnancy proceeded uneventfully to 39 weeks, terminating in the birth of a healthy male infant of 3680 grams.
Discussion
Incidence
Heterotopic pregnancy is an unusual and problematic type of ectopic pregnancy. Historically, the incidence of heterotopic pregnancy was estimated as 0.3:10,0001. However, in the last twenty years there has been an almost four‑fold increase in the incidence of ectopic pregnancy in the general population and a corresponding increase in the incidence of heterotopic pregnancy. This increase has been attributed to:
· increase in the incidence of pelvic inflammatory disease;
· prevalent use of IUDs;
· increase in tubal surgery, notable microsurgery;
· pharmacologic ovulation stimulation;
· assisted reproductive techniques
Each of these risk factors increases the risk for ectopic pregnancy from 2‑7 times above that of the general population, with pelvic inflammatory disease having the most significant effect10.
Consequently, a more recent re‑evaluation of the incidence of heterotopic pregnancy in the general population presents a fairly conservative estimate for its incidence as 1.25:10,000 pregnancies2.
Within the population with risk factors for ectopic pregnancy, the incidence is considerably higher. Patients with pelvic inflammatory disease are estimated to have a risk of 2.5‑6.25:10,000 for heterotopic pregnancies.
In addition, recent evidence from research in reproductive technology indicates that heterotopic pregnancy occurs even more frequently in patients participating in ovarian induction programs, where an incidence of 33:10,000 has been reported4.
Furthermore, as Goldman et al pointed out, the risk of heterotopic pregnancy appears to be even greater after assisted reproductive technology (IVF or GIFT) has been used. Their data supports other evidence that the risk in this patient population approaches 100:10,0005.
Clearly, the historical estimate of the incidence of this "rare" condition does not reflect our modern experience. Within certain recognized subgroups of the obstetric population heterotopic pregnancy is not a rare entity and should be high on the list of differential diagnoses.
Diagnosis
Earlier diagnosis and treatment of ectopic pregnancies has resulted in a dramatic decrease in maternal morbidity and mortality in spite of the increasing incidence of the condition. The application of rapid quantitative assays for the beta subunit of hCG combined with the use of transvaginal ultrasound has significantly contributed to this earlier diagnosis.
For example, at our institution, we expect to see a normal intrauterine gestation when the b‑hCG reaches a level of 1700 mIU/mL (First International Preparation). This would correspond to a menstrual age of 6.5 weeks. Failure to see an intrauterine gestation at this level raises the suspicion of an abnormal pregnancy—particularly an ectopic pregnancy.
Other pelvic findings will increase or even confirm this suspicion. Finding a live embryo in the adnexa is 100% specific for an ectopic pregnancy. However, this finding occurs in only 10% of ectopic pregnancies13. An adnexal mass is seen in 60‑90% of ectopics and specifically raises suspicion of an ectopic pregnancy if the mass is seen to be separate from the ovary. Gentle pressure with the transducer can help confirm this. A significant amount of free fluid is also suspicious, especially if the fluid is echogenic. However, these latter two findings are nonspecific and can also be seen with other adnexal pathology such as a hemorrhagic corpus luteum, ovarian inflammation, ovarian torsion and appendicitis.
It is the presence of the intrauterine gestation that makes the diagnosis of a heterotopic pregnancy more problematic than the diagnosis of other types of ectopic pregnancy.
In other types of ectopic pregnancy, the serum b‑hCG tends to be lower than a normal intrauterine pregnancy of the same menstrual age. Serial assays demonstrate a delayed doubling time. However, unlike other forms of ectopic pregnancy, a heterotopic pregnancy demonstrates normal b‑hCG values due to the presence of the normal intrauterine gestation. Thus, in the diagnosis of heterotopic pregnancy the b‑hCG assay is useful, when negative, to rule out an ectopic, but is not helpful, when positive, to suggest the presence of a heterotopic gestation. Also, in other types of ectopics, the index of suspicion is raised by the nonvisualization of an intrauterine pregnancy when the b‑hCG exceeds a threshold level. Conversely, the presence of an intrauterine gestational sac lowers the suspicion of an ectopic pregnancy. Thus, the visualization of an intrauterine gestation may result in less rigorous sonographic evaluation of the adnexae and a delayed or missed diagnosis of a heterotopic gestation.
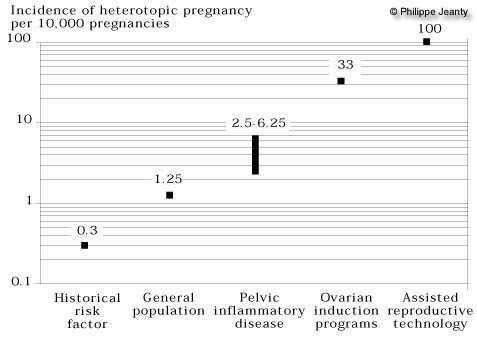
Figure 7: Frequency of heterotopic pregnancy, per 10,000 pregnancies, among several groups at risk.
In all other types of ectopic pregnancy, the nonvisualization of an intrauterine gestation when the b‑hCG exceeds 1700 mIU/mL (First International Preparation) is a strong indicator of ectopic pregnancy. The adnexal and extrauterine findings are then used to support or challenge the diagnosis.
In a heterotopic pregnancy, only careful examination of the extrauterine anatomy provides the means of making the sonographic diagnosis.
Sonographically, an adnexal mass is seen in 80% of ectopic pregnancies. In 20% of ectopics, no sonographic evidence of an adnexal mass is found. It is reasonable to expect that these percentages can also be applied to heterotopic pregnancies. This means that in 20% of cases the sonographic diagnosis of a heterotopic pregnancy cannot be made. Conversely, however, it also means that potentially the diagnosis can be made in 80% of the cases with rigorous sonographic evaluation of the adnexae. Suspicious adnexal masses can be investigated with Doppler ultrasound in an attempt to improve sensitivity and specificity. Taylor and coworkers have described a high velocity, low resistance Doppler signal that is associated with the developing trophoblast15 . They report that identification of this type of flow pattern in an adnexal mass using transabdominal ultrasound raised the sensitivity for the diagnosis of an ectopic pregnancy from 53% to 73%. They also report a sensitivity of 96% and a specificity of 93% using transvaginal color Doppler. We are currently using transvaginal color Doppler to assess all suspected ectopics, but, as yet, have been unable to see such encouraging results.
Management
Surgical removal of the ectopic gestation by salpingectomy or salpingostomy is the treatment of choice. In patients in whom the diagnosis of ectopic pregnancy can be made without laparoscopy and who sonographically demonstrate an unruptured gestation and a persistent downward trend to the b‑hCG assay, expectant management has been successfully applied16. This form of conservative management can also be applied to heterotopic pregnancies having a similar clinical appearance. Salpingocentesis with the introduction of methotrexate or potassium chloride into the gestational sac is investigational at this time. There is at least one report of its successful application in the management of a heterotopic pregnancy17.
Summary
Heterotopic pregnancy, once thought to be an extremely rare phenomenon, is becoming more common as the overall incidence of ectopic pregnancies continues to increase.
The diagnosis of this potentially dangerous form of ectopic pregnancy is difficult and is often delayed. In patients with risk factors for ectopic pregnancy rigorous sonographic examination of the adnexae and cul de sac must always be made even in the presence of an intrauterine gestation if the diagnosis is going to be made sonographically. Such investigation must employ high resolution transvaginal transducers and meticulous technique. Doppler ultrasound may also be helpful.
In patients without risk factors, the presence of an intrauterine gestation much more reliably excludes the possibility of a heterotopic gestation, but does not rule it out. As this case demonstrates, whenever abnormal adnexal findings are demonstrated and the b‑hCG is positive, the possibility of a heterotopic pregnancy must be entertained.
References
1. DeVoe RW, Pratt JH: Simultaneous intrauterine and extrauterine pregnancy. Am J Obst Gynecol 56:1119, 1948.
2. Richards SR, Stempel LE, Carlton BD: Heterotopic pregnancy: Reappraisal of incidence. Am J Obst Gynecol 142:928, 1982.
3. Bello GV, Schonolz D, Moshirpur J, et al: Combined pregnancy: The Mount Sinai experience. Obstet Gynecol Surv 41:603, 1986.
4. Yovich JL, McColm SC, Turner SR, et al: Heterotopic pregnancy from in vitro fertilization. J in Vitro Fert Embryo Transf. 2:146, 1985.
5. Goldman GA, Fisch B, Ovadia J, et al.: Heterotopic pregnancy after assisted reproductive technologies. Obstet Gynecol Surv 47:217, 1992.
6. Molloy D, Deambrosis W, Keeping D, et al.: Multiple‑sited (heterotopic) pregnancy after in vitro fertilization and gamete intrafallopian transfer. Fertil Steril 53:1068, 1990.
7. Dor J, Seidman DS, Levran D, et al: The incidence of combined intrauterine and extrauterine pregnancy after in vitro fertilization and embryo transfer. Fertil Steril 55:833, 1991.
8. Berger M, Taymor M: Simultaneous intrauterine and tubal pregnancies following ovulation induction. Am J Obstet Gynecol 113:812, 1972.
9. Mattingly RF, Thompson JD: Te Linde"s Operative Gynecology 6th Edition; Philadelphia: J.P. Lippincott, 1985:444.
10. Westrom L: Incidence, prevalence and trends of acute pelvic inflammatory disease and its consequences in industrialized countries. Am J Obstet Gynecol 1980; 138:880‑892.
11. Attrash HK, Friede A, Hogue CJ.: Ectopic pregnancy mortality in the United States, 1970‑1983. Obstet Gynecol 70:817, 1987.
12. Neiger R, Gailey S, Wall AM, et al: Diagnosis of ectopic pregnancy using transvaginal ultrasound scanning. JReprod Med 34:52, 1989.
13. Cartwright PS: Diagnosis of ectopic pregnancy, Obstet Gynecol Clin North Am 18:1, 1991.
14.Pittaway DW, Wentz AC, Mason WS, et al: The efficacy of early pregnancy monitoring with serial chorionic gonadotropin determinations and real‑time sonography in an infertile population. Fertil Steril 44:190, 1985.
15. Taylor KJ, Ramos IM, Feyock AL, et al: Ectopic pregnancy: Duplex Doppler evaluation. Radiology 173:93, 1989
16. Stoval TG, Ling FW: Expectant management of ectopic pregnancy: Obstet Gynecol Clin North Am 18:1, 1991, 135‑143.
17. Robertson EE, Moye MA, Hanse JN, et al: Reduction of ectopic pregnancy by injection under ultrasound control. Lancet 1:974, 1987.